Dr. Martin McCaffrey | May 16, 2013 | SHARE: 


DOWNLOAD ENTIRE ARTICLE (with images and endnotes)
Kia was 20 years old, in her second year of college, and 23 weeks pregnant when her previously normal pregnancy radically changed. One morning she felt a gush of fluid followed by painful contractions. She rushed to a nearby emergency room, where she was told she was in preterm labor and her baby might deliver early. Kia was transferred to a larger nearby hospital, admitted and started on magnesium to try and stop her labor. Despite the doctor’s best efforts over an exhausting three days, her labor did not stop. Kia delivered Milo, a 1 pound 3 ounce baby boy who fit in the palm of his father’s hand. Over the next four months as Milo battled severe premature lung problems, three weeks on a ventilator, surgery for premature eye disease, and severe bleeding in the brain, Kia kept watch at Milo’s bedside. She asked me twice during Milo’s hospitalization, “Why did this happen to us? I didn’t smoke, ate right and took my vitamins.” Kia and I spoke one last time as she prepared to take Milo home. She had five follow-up appointments confirmed and was an expert at giving Milo his four medications. The tanks Milo would need to provide him with oxygen at home had been delivered. College was on the backburner now, and Kia was very aware that she and Milo were starting on a challenging journey. Tearful, Kia thanked me and the staff that had cared for Milo, and said, “I sure hope you doctors will figure out one day how we can keep babies from coming early.”
Prematurity, defined as a birth prior to 37 weeks gestational age, is one of the most challenging public health issues in America. Nearly 12 percent of all babies born in the United States are born preterm. In North Carolina 10.4 percent of births, 12,750 babies, were born preterm in 2011. Preterm birth may be preceded by early rupture of membranes or preterm labor. This leads to hospitalizations of days or weeks for mothers as doctors attempt to try and prevent an early delivery. In the case of a very preterm birth (VPB), defined as an infant born at less than 32 weeks gestation, hospitalizations from 4-16 weeks can be expected. While keeping vigil at the bedside, many mothers will see their baby have a breathing tube placed, live on a ventilator for days to weeks, intravenous lines inserted in the belly button and veins, and feedings delivered through feeding tubes. A mother may watch helplessly as her baby develops life-threatening infections or conditions requiring surgery. After days or weeks of struggling, this heroic infant may be one of the 20 percent that does not survive. As staggering as the emotional and social toll of this epidemic is, equally devastating is the financial impact. The estimated annual cost for care attributable to preterm birth in the United States is $26 billion.1
Over the last two decades, the percentage of preterm deliveries has risen 20 percent.2 Annually in the U.S., 80,000 births are classified as VPB. VPBs constitute two percent of all births,3 and in developed nations, VPB is the leading cause of death in newborns. While medical advances have allowed infants as young as 22 weeks gestation to survive, the chances for survival diminish with decreasing gestational age. The VPB infants that do survive are at risk for lifelong complications, including breathing problems, cerebral palsy, autism, blindness and mental retardation.
Preterm birth does not have a single identifiable cause, but it has been associated with a number of factors. In 2006, the Institute of Medicine (IOM) published one of the most comprehensive reviews of preterm birth ever compiled. It identified prior preterm birth, incompetent cervix, multiple gestation pregnancy, infection, and smoking as some of the factors associated with preterm birth. An “association” is defined statistically by methods that exclude the possibility that the apparent relationship of a factor with an outcome of interest occurs by chance. If statistics exclude chance as an explanation for the association, then there is a real association, and investigators turn to analyzing whether the associated factor is possible cause for the outcome. The relationship between smoking during pregnancy and preterm birth illustrates the concept of “association.” While an association has been reported to exist between smoking and preterm birth, preterm birth does occur in mothers who do not smoke. Similarly, all mothers who smoke do not experience preterm birth. Smoking during pregnancy, according to some studies, is associated with an increased likelihood of preterm birth; but not all studies have reached this conclusion. The IOM report concluded:
Many studies have examined the association between smoking and preterm birth, and they generally find modest associations. Recent studies continue to show such a pattern. However, some reports suggest a stronger association and others suggest no association at all.
Despite just a “modest association,” and lack of proof of probable causality, public health experts have identified smoking as a modifiable risk factor that might reduce a mother’s risk for delivering a preterm baby. As a result, the U.S. Surgeon General in 1985 determined it was his duty to warn mothers who smoked of the association with an increased risk for a preterm birth. The concern regarding this association remains significant enough that the Surgeon General’s warnings on cigarette packages issued in 1985 continue to this day: “Smoking By Pregnant Women May Result in Fetal Injury, Premature Birth, And Low Birth Weight.”
Safety. Another association with preterm birth which is scientifically established, but less publicized, is a prior abortion. In this article, “abortion” refers solely to induced abortion or termination of pregnancy, not spontaneous abortion. Introduced into clinical practice in 1958, vacuum or suction aspiration has become the most commonly performed abortion procedure. One might assume that the introduction of this technique followed animal safety studies and other clinical trials evaluating the potential impact of suction aspiration. Such has been the case since 1947 when, reeling from the horrors of Nazi medical experimentation, international agreements were signed at Nuremberg that required a new medical treatment be first tested on animals before human experimentation. Some might be surprised to find that this was not the case with suction abortion. In 1958, Chinese physicians published the use of a new technique requiring a new device, suction abortion, which they had performed on 300 Chinese women. It is incomprehensible for us today to imagine physicians introducing a new surgical technique and device, and presuming it was without potential harm, dismissing the need for safety testing in animal and clinical trials. That, however, is exactly what happened in the case of one of the most commonly performed surgical procedures in the world, suction aspiration abortion. Suction abortion has no published animal studies; there are no clinical studies designed to validate its short and long term safety.
While abortion providers have not provided safety data validating that it is free from adverse effects, the widespread use of abortion has demonstrated that abortion is associated with at least one severe reproductive health outcome: a risk of future preterm birth. To date, 137 studies have demonstrated this association. The association between prior abortion and future preterm birth is strongest for the most premature of births. Twenty four studies have shown a statistically significant increase in the risk for VPBs or very low birth weight (VLBW defined as birth weight less than 1500 grams). Nine studies have demonstrated the association of abortion with extremely preterm birth (births less than 28 weeks’ gestation). Many of these studies demonstrate a risk for preterm birth that incrementally increases with a history of increasing numbers of prior abortions. This increased risk for preterm birth with increased exposure to abortion is referred to as the dose-response relationship between abortion and preterm birth.
Studies and the Data. Medical journals print thousands of studies annually. The challenge is to determine which studies reach clinically significant conclusions. One study, however, even if highly significant, cannot definitively establish an association as a real risk or probable cause. If a variable is a real risk, the relationship will be reproducible in other studies. The gold standard in establishing the strength of such a relationship is the systematic review with meta-analysis (SRMA). The systematic review (SR) provides an exhaustive summary of literature relevant to a research question; it uses an objective approach for the evaluation of studies on the topic with the aim of minimizing bias in those studies included in the final meta-analysis. The meta-analysis (MA) then combines results from different studies with the intent of identifying whether there is a consistent association of a factor with an outcome.
In 2009, two well-designed SRMAs were published that reviewed the world’s literature on the association of abortion with preterm birth. These studies ultimately incorporated a total of 41 studies in their analyses, and demonstrated not only an association of prematurity with one induced abortion, but a dose-dependent further increase in risk for mothers with a history of two or more abortions. The first study, by Swingle et al., determined that a single prior abortion increased the risk of a future VPB by 64 percent. The second study, by Shah et al., reported that a single prior abortion increased the risk of preterm birth by 36 percent, while more than one abortion increased the risk for preterm birth by 93 percent. This latter finding indisputably established that when a woman has increasing numbers of abortions, her risk for preterm birth increases further. This is a dose-dependent response association. Over the last two years, large national studies from Finland and Scotland provided further evidence of the abortion-prematurity association.14 More recently, researchers in Canada published the results of an analysis reporting that women with one abortion were 45 percent, 71 percent, and 217 percent more likely to have premature births at 32, 28, and 26 weeks. This risk was stronger for women with two or more previous abortions. Arrayed against this overwhelming evidence of the abortion and preterm birth association are NO SRMAs to dispute the abortion and preterm birth association.
Statistical analysis has definitively shown that the relationship between abortion and prematurity is not due to chance. The association is established. The next step then is to ask the question, “Is a prior abortion a cause for some future preterm births?” The criteria for establishing probable cause require moving beyond statistical analysis. Hill’s “Criteria of Causation” describes the minimal conditions needed to establish a causal relationship between two items.16 These conditions include a temporal relationship, dose-dependent response, biologic plausibility, consistency and strength of association. A review of these criteria for the abortion-preterm birth link demonstrates the following:
Abortion is linked not only with preterm birth, but it is even more strongly linked with VPB. There is strength of association.
The association of abortion with preterm birth is consistently stronger than the association of preterm birth and maternal smoking. Objective review of the literature not only establishes the strength of the abortion and preterm birth association, it also reveals that prior abortion satisfies criteria as a probable cause, though not the only cause, for a future preterm birth.
The Experts Weigh In. Expert opinion has openly acknowledged that the evidence demonstrates the association of abortion with preterm birth. Dr. Jay Iams, maternal fetal medicine specialist, world renowned authority on prematurity and IOM Preterm Birth Committee member, stated in 2010:
Contrary to common belief, populationbased studies have found that elective pregnancy terminations in the first and second trimesters are associated with a very small but apparently real increase in the risk of subsequent spontaneous preterm birth.
Dr. Phil Steer, Editor of the British Journal of Obstetrics and Gynecology, commenting on the 2009 Shah study editorialized:
A key finding is that compared to women with no history of termination, even allowing for the expected higher incidence of socio-economic disadvantage, women with just one TOP (termination of pregnancy) had an increased odds of subsequent preterm birth. We have known for a long time that repeated terminations predispose to early delivery in a subsequent pregnancy. However the finding that even one termination can increase the risk of preterm birth means that we should continue to search for ways of making termination less traumatic.
The previously mentioned IOM Report on Prematurity in 2006 noted the association of abortion with prematurity. The IOM identified abortion as an “immutable” risk factor for preterm birth. This characterization defined a history of abortion as an unchangeable element in a women’s risk profile for future preterm birth and no recommendations were made regarding informing the public about this association. The fact is we do not know if this association is immutable. Once an abortion has occurred it might remain an immutable risk factor for future preterm birth. However, the association of abortion with prematurity could be similar to the risk of lung cancer developing as a result of smoking. If the behavior or exposure ends, over time the risk for an unwanted morbidity (lung cancer and perhaps preterm birth) wanes. One thing is for certain, while it is unclear whether or not abortion is a lifelong immutable risk factor for preterm birth, it is indisputable that measures which reduce rates of initial or subsequent abortions will reduce the likelihood of a woman having a future preterm birth.
Is information regarding the increasing risk for a future preterm birth with increasing numbers of abortions important for women of childbearing age in North Carolina who have had a prior abortion? Is this important information for women of childbearing age who have not yet had an abortion, but consider abortion a potential method for family planning? In an era of informed consent in which many patients feel it is their right to know the potential risks for medical procedures, the answer is obvious.
This information is especially important, given that abortion is one of the most commonly performed surgical procedures, and it has significant potential impact on the future reproductive health of a young woman. In dealing with legislation regarding a politically charged topic like abortion, however, some might demand to know what the real impact of the association between abortion and prematurity is for the citizens of North Carolina.
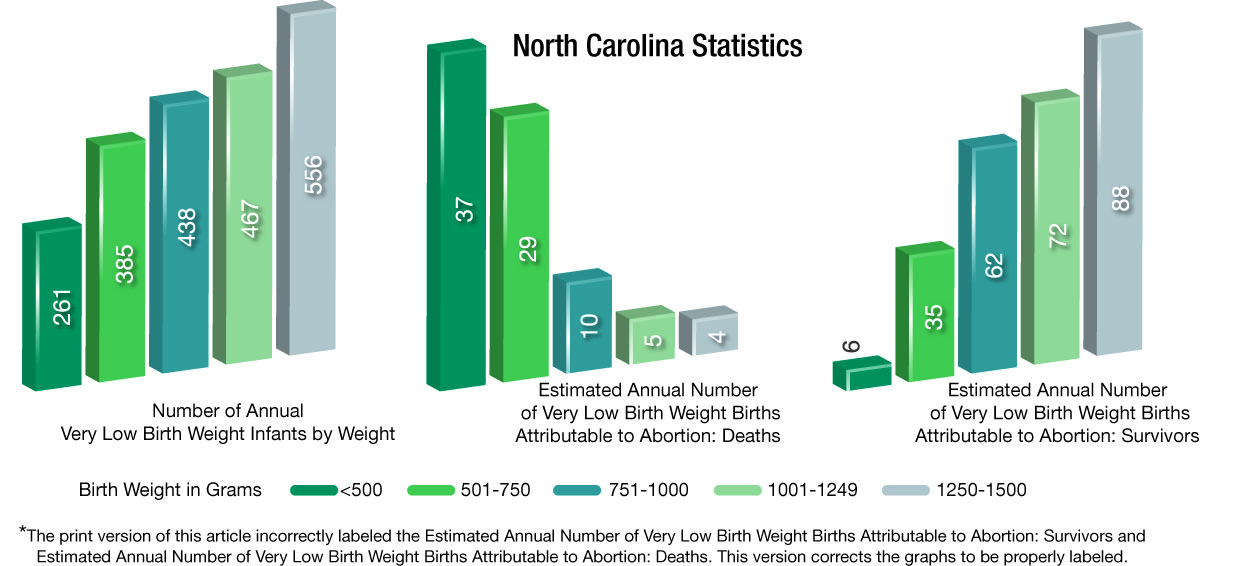
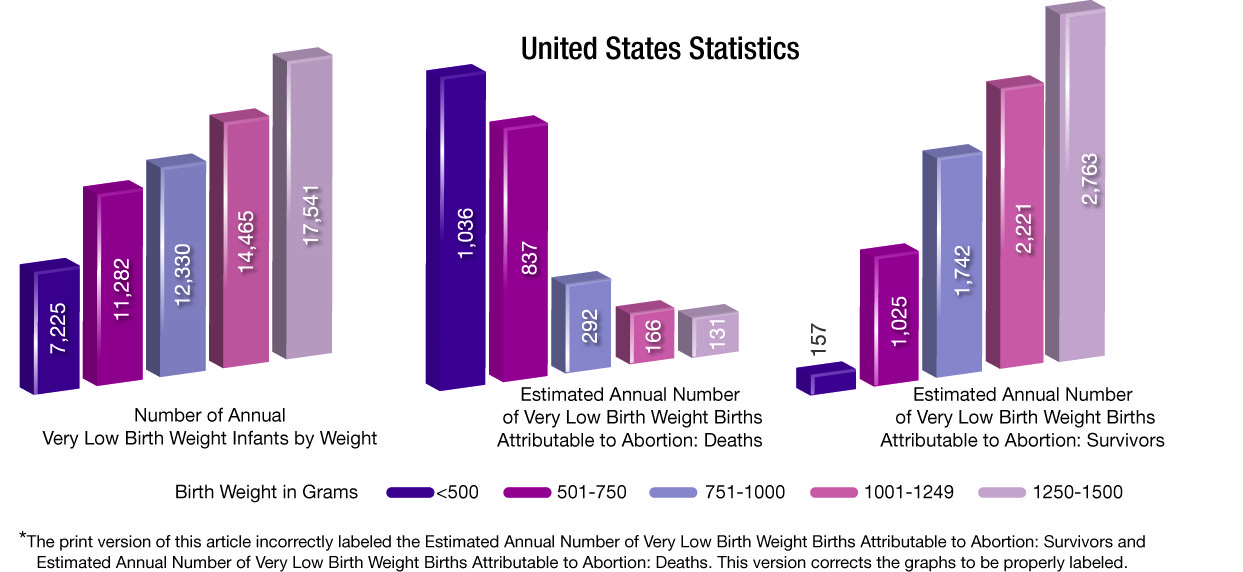
Fiscal. An analysis of the impact of the abortionprematurity association in North Carolina was performed in 2008 by the General Assembly.20 This analysis is based on a cost analysis of abortion published by Calhoun et al.21 Updating this analysis for the data reported by Swingle et al.22 and North Carolina data,23 adjusted for 2013 costs, reveals the following estimates:
Racial Disparity. A focus for healthcare providers and public health officials in North Carolina is the disparity in health outcomes that exist between the white, black and Hispanic communities. While all races share in the prematurity epidemic and the association of prematurity with abortion, the impact on the Hispanic community tracks closest to the white community while the black community is most profoundly affected. Based on 2010 North Carolina State Center for Health Statistics data, the latest data available, VPB birth affects blacks at a rate 2.5 times higher than whites. The 2011 data from NC State Center for Health Statistics Pregnancy Data reports that North Carolina blacks used abortion services at a rate that is three times that of whites.24 This historically consistent pattern of increased use of abortion services in blacks creates a significant disparity in their risk for VPB. Based on this data, of the 262 VPBs estimated to occur annually in North Carolina in association with abortion, 110 of these births can be expected to occur among black mothers having 28,509 live births. Of the 262 very preterm births associated with abortion, the same number, 110, will be born to white mothers having 67,542 live births. In summary, VPBs with an abortion association represent 1.10 percent of black births in North Carolina and 0.46 percent of white births. The racial disparity is clear.
The abortion-preterm birth association is news to many, despite the fact that the literature regarding this link is larger and stronger than that for other commonly accepted associations with prematurity. The most profound illustration of this gap in public knowledge is the fact that cigarettes are labeled with warnings from the Surgeon General regarding the potential impact of smoking on preterm birth. There is no SRMA of smoking and preterm birth reporting a 36 percent increased risk of preterm birth from smoking one-half pack of cigarettes a day, or a 93 percent increased risk from smoking one pack per day.
In concluding their landmark SRMA publication on the abortion-prematurity association, Shah et al. state:
More than a million abortions are performed in the US per year. Of these, more than 75 percent of women wish to or get pregnant again. These women should know the risks associated with I-TOP (induced abortion) not only for their health but also for their future reproductive potential. A properly obtained consent legally mandates explanation of these risks to women and ensuring their understanding. Potential areas for knowledge transfer include education of girls and women enrolled at schools or colleges, during routine visits to family doctors or specialists, and finally when counseling women seeking abortion.
Given the strength of the evidence demonstrating the abortion-preterm birth link, one might expect providers of abortion services to have learned from the tobacco industry and proactively inform patients of the impact their services might have on future health. This is not the case. Planned Parenthood, the leading provider of abortion services in the nation, has consistently dismissed and denied the incontrovertible evidence that abortion increases a woman’s risk for preterm birth. Despite the abortion-preterm birth association being scientifically established, Planned Parenthood states on their national website, “Safe, uncomplicated abortion does not cause problems for future pregnancies such as birth defects, premature birth or low birth weight babies, ectopic pregnancy, miscarriage, or infant death.”
The decision by women of child bearing age to have an abortion can have profound a impact on future pregnancies and their future family. The gap in public knowledge that currently exists, and the prevalence of abortion in North Carolina, mandates that those concerned with public health take steps to inform North Carolina women and their partners about the risks abortion poses for a future preterm birth. Senate Bill 132—Health Curriculum/ Preterm Birth (S132) is a small step in that direction. S132, sponsored by Senators Warren Daniel (R–Burke), Jerry Tillman (R–Moore), and Shirley Randleman (R–Stokes), along with three co-sponsors, is supported by the North Carolina Child Fatality Task Force (CFTF). S132 would add to the current School Health Education Program information on the preventable factors associated with preterm birth, including the risk abortion poses for preterm birth in subsequent pregnancies. S132 capitalizes on the opportunity to better inform young women and men who are making decisions related to their sexual behavior which may have lifelong implications. The education advocated by S132 may lead some young women and men to reconsider their sexual and other lifestyle choices before they make decisions which impose significant future risk for preterm birth. S132 will be an important part of ongoing state education efforts that will hopefully lead significant numbers of students to make more responsible choices.
Everyone should hope that abortion becomes an increasingly rare event. The education provided for in S132 can contribute significantly to making this hope a reality. Over time, as the use of abortion services decreases, North Carolina will see a reduction in preterm and VPB rates, a reduction in the disparity of black VPBs, and a decline in the enormous challenges preterm birth places on the healthcare system and North Carolina families.
DOWNLOAD ENTIRE ARTICLE (with images and endnotes)
Martin McCaffrey, M.D., is a clinical professor of pediatrics at the UNC-Chapel Hill School of Medicine, director of the Perinatal Quality Collaborative of North Carolina, and member of the N.C. General Assembly Child Fatality Task Force.